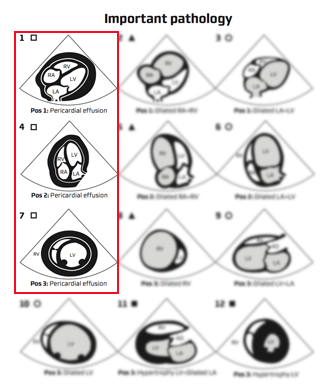
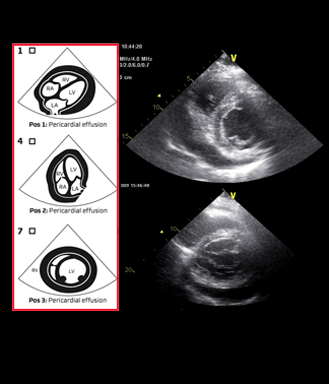
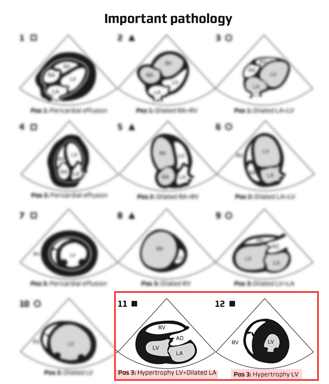
Video clips of the parasternal short axis view
Notice:
– Enlarged RV
– D-shaped left ventricle
– Paradoxial movement of the interventricular septum
– Arrows pointing to dilated right ventricle
Right ventricle enlargement and myocardial dysfunction is seen in right side myocardial infarction and pressure increase (pulmonary embolus and chronic pulmonary hypertension)
In acute enlargement the high pressure in the right ventricle will compress the left ventricle resulting in typical paradoxial interventricular septal movement and D-shape of the left ventricle