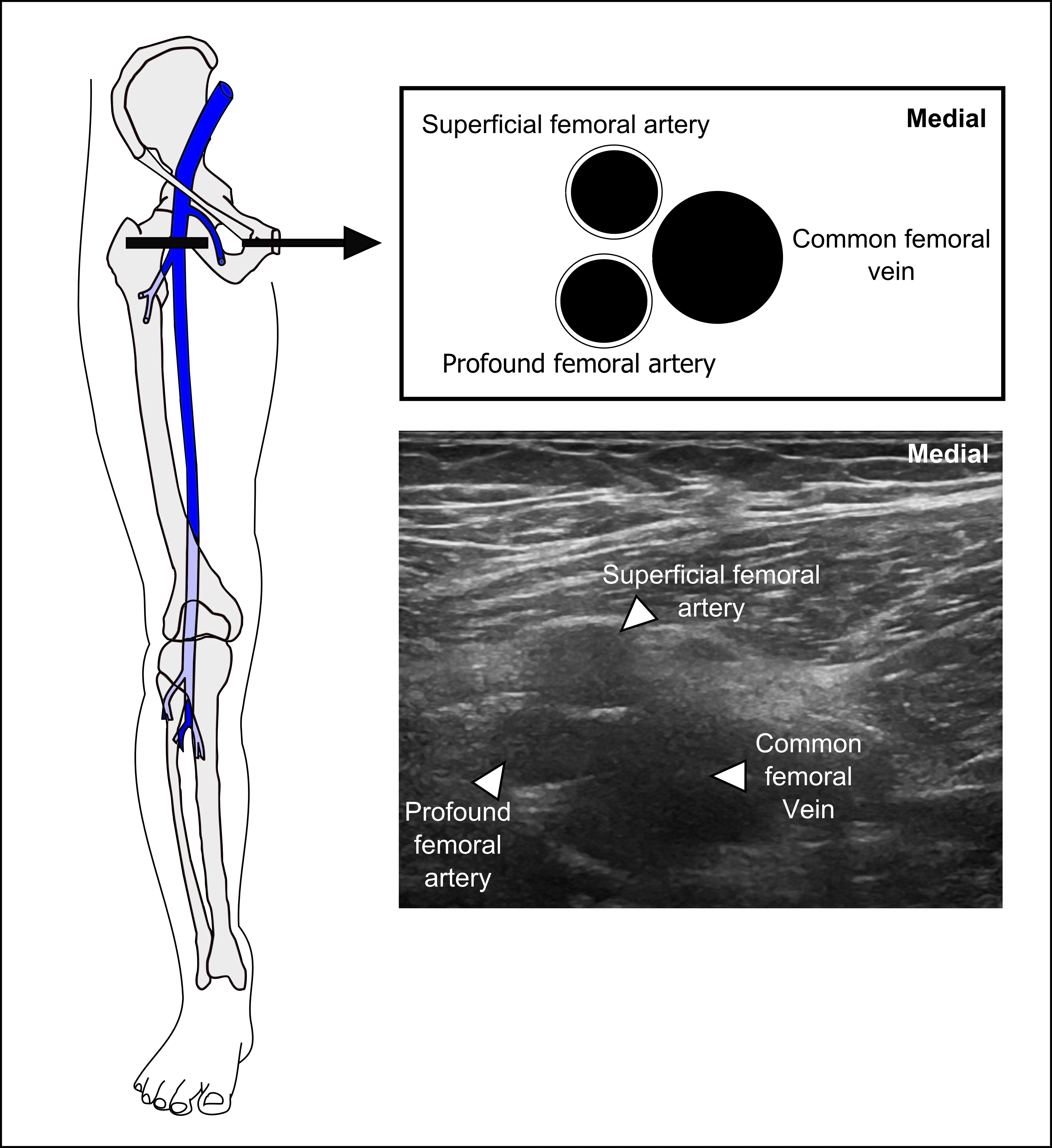
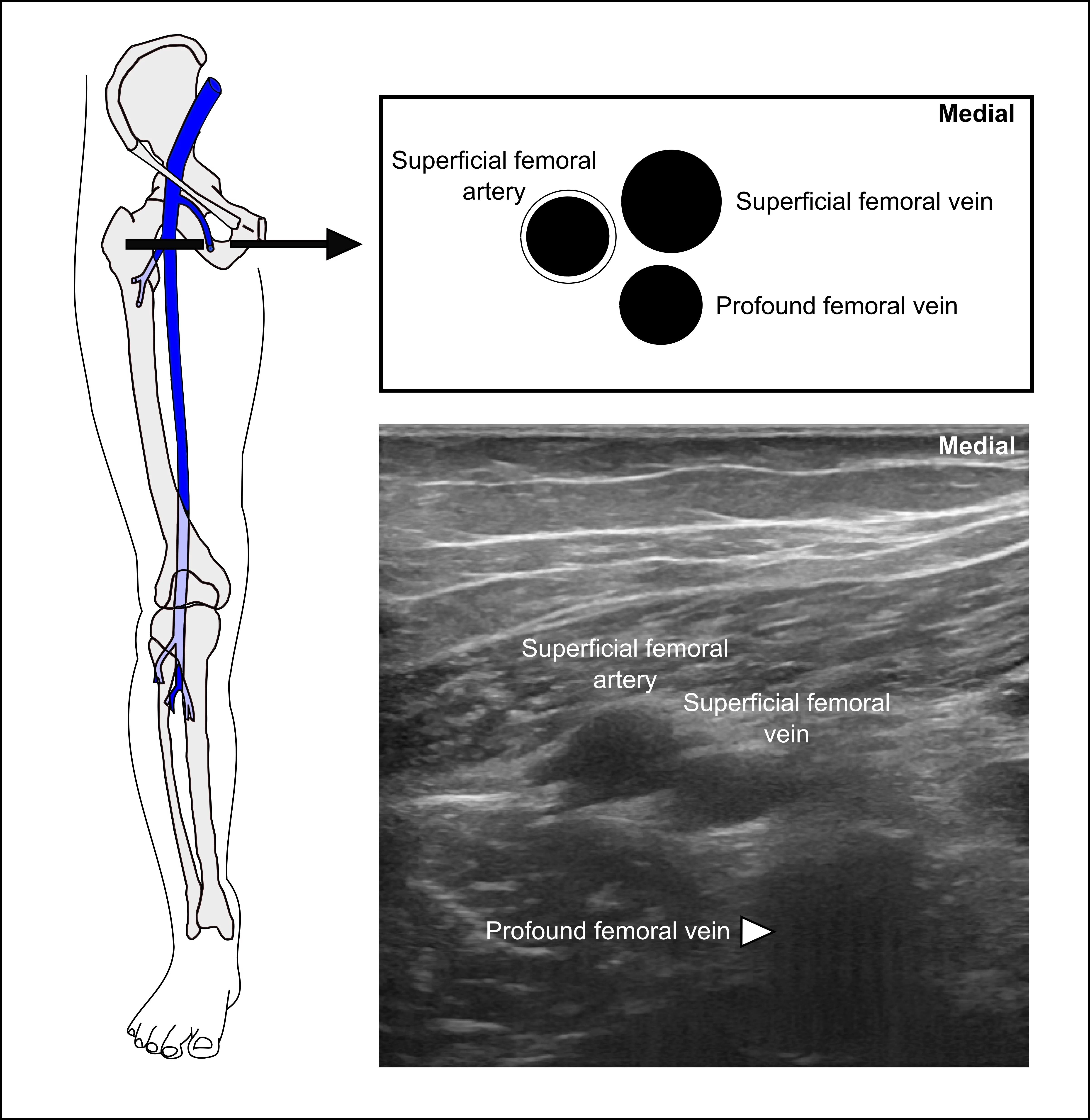
Next, the physician will sweep the ultrasound probe distally to image the bifurcation of both the common femoral vein and common femoral artery. There is anatomical variation as to which bifurcates first. The pictures here demonstrate that variability.
Note: Deep femoral artery and profound femoral artery are synonyms. Deep femoral vein and profound femoral vein are synonyms.