In emergency cardiac ultrasonography no precise measurements or advanced knobology is needed.
A simple visual qualitative method to evaluate the overall function of the heart and chambers is used.
This method is called eyeballing.
All views can be used for the eyeballing and combined information from different views is recommended.
When eyeballing, always apply suitable humbleness.
Eye-balling for each focused question will be described in further detail.
Tips and tricks
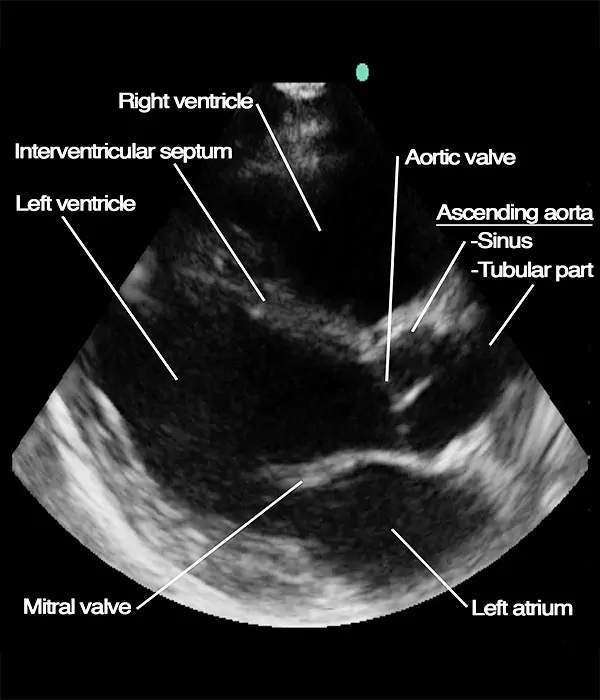
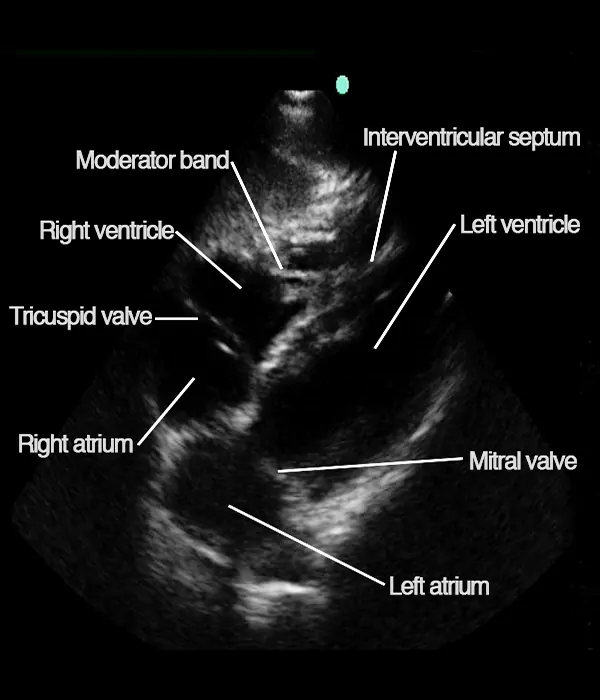
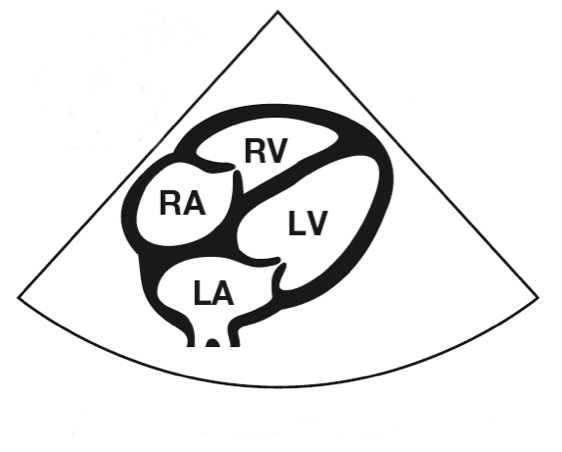
The result of eyeballing the 4 cardiac views below would be: no pericardial effusion, no signs of Type A aortic dissection present, normal left ventricular function, no signs of pulmonary embolism present.