The infraclavicular brachial plexus block anaesthetize all the bones and joints of the upper limb distal to the shoulder:
– The axillary nerve innervates the head of the humerus
– The radial nerve innervates the arm, the elbow, the forearm, the hand and the
radial fingers
– The musculocutaneous nerve innervates the humerus
– The ulnar nerve innervates the elbow and the hand and the ulnar fingers
– The median nerve innervates the elbow and the forearm and the hand and the
radial fingers
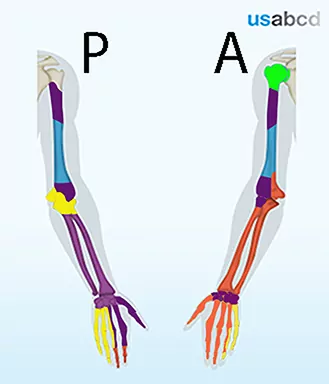
blue = musculocutaneous nerve; yellow = ulnar nerve; orange = median nerve