If the perineural spread of local anaesthetic is not perfect, the needle can be relocated in real-time before injection of the remaining local anaesthetic
Click on the VIDEO CLIP button to view the video
Relocate the needle tip if necessary to obtain perineural spread of local anaesthetic
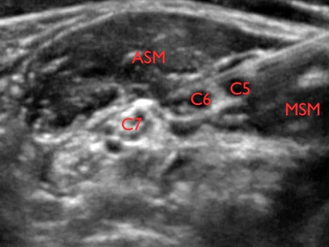
C5 = spinal nerve root of C5; C6 = spinal nerve root of C6 (2 profiles); ASM = anterior scalene muscle; MSM = middle scalene muscle
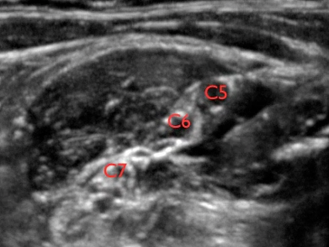
Another example of relocation of the needle tip to obtain the endpoint of spread of local anaesthetic alongside the spinal nerve branches of C5 and C6
Click on the VIDEO CLIP button to view the video
The video demonstrates relocation of the needle tip in order to cover the C5 and C6 spinal nerve branches with local anaesthetic in the interscalene groove
C5 = spinal nerve root of C5; C6 = spinal nerve root of C6; C7 = spinal nerve root of C7; A = small artery
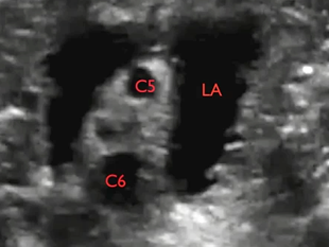
When local anaesthetic is injected it generates a contrast effect that enhances visualisation of the target nerves, because of the black background of the fluid
Click on the VIDEO CLIP button to view the video
Bright are the stars that shine. Dark is the sky
C5 = spinal nerve root of C5; C6 = spinal nerve root of C6; LA = local anaesthetic
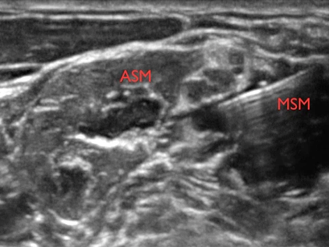
It is important to advance the needle tangential to the target nerves and NOT penetrate the nerves
Click on the VIDEO CLIP button to view the video
By advancing the needle tangentially to the nerves, it is possible to avoid piercing the nerves
C5 = spinal nerve root of C5; C6 = spinal nerve root of C6; C7 = spinal nerve root of C7; ASM = anterior scalene muscle; MSM = middle scalene muscle
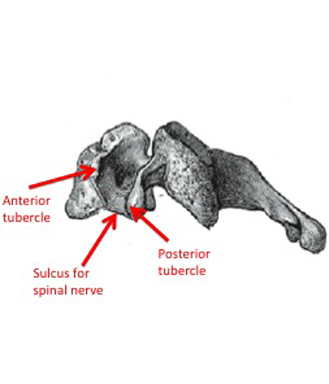
It is possible to follow the spinal nerve roots all the way to the sulcus for the spinal nerve of the transverse process of the appertaining cervical vertebra
The seventh cervical vertebra does not have an anterior tubercle
A drawing of the fourth cervical vertebra showing the sulcus for spinal nerve at the end of the transverse process between the anterior tubercle and the posterior tubercle
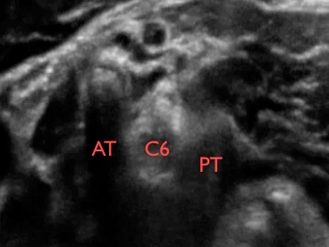
Each spinal nerve can be tracked from the branches of the brachial plexus in the transition zone behind the subclavian artery on top of the first rib to the sulcus of the spinal nerve of each transverse process
Click on the VIDEO CLIP button to view the video
The video shows tracking of C8, C7, C6 and C5 to their sulci on the transverse processes
AT = anterior tubercle; PT = posterior tubercle; C5, C6, C7, C8, and T1 = the spinal nerve roots of the brachial plexus
The in-plane approach to the interscalene brachial plexus block
Local anaesthetic is deposited lateral to C5 and C6
You often feel a “pop” as you enter the interscalene groove
Click on the VIDEO CLIP button to view the video
The video shows the in-plane approach to the interscalene block of the brachial plexus
ASM = anterior scalene muscle; MSM = middle scalene muscle; C5 = spinal nerve root of C5; C6 = spinal nerve root of C6
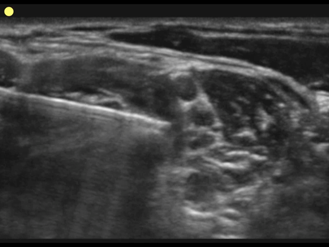
To localise the brachial plexus you should start by localising the pulsating subclavian artery where it runs across the first rib
The branches of the brachial plexus are located just lateral to the artery
Track the branches of the brachial plexus proximally until they line up as a string of black pearls in the interscalene groove
Click on the VIDEO CLIP button to view the video
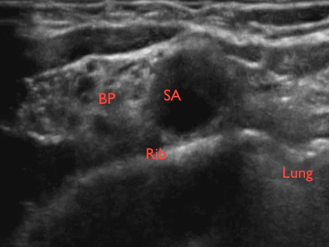
The video shows the tracking of the branches of the brachial plexus from the level of the subclavian artery to the interscalene groove
SA = subclavian artery; BP = cluster of branches of the brachial plexus; ASM = anterior scalene muscle; MSM = middle scalene muscle
– Insert the needle from the posterior end of the probe
– Empty the hose and the needle of air by injecting 1/2 mL of local anaesthetic subcutaneously before advancing the needle
– Advance the needle with in-plane technique until the needle tip touches the lateral side of the BP between C5 and C6
– The endpoint of injection is complete spread of local anaesthetic along the lateral side of the C5 and C6 spinal nerve branches
– Reposition the needle tip as necessary to reach the endpoint
The in-plane approach to the interscalene brachial plexus block
The in-plane approach is recommended as the first choice, as it allows real-time control of the position of the needle tip at all times
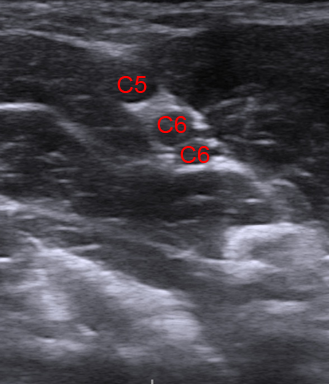
At the top of the interscalene groove the brachial plexus presents as the C5 and the C6 spinal nerve branches – and usually the C6 is split in two branches
The three profiles of C5 and C6 are usually lined up like a string of black pearls sandwiched between the anterior scalene muscle and the middle scalene muscle
The string of black pearls made up by the spinal nerve branches of C5 and C6