Surgery and analgesia of the upper limb distal to the shoulder level
The ultrasound guided infraclavicular brachial plexus block is a basic level block

Surgery and analgesia of the upper limb distal to the shoulder level
The ultrasound guided infraclavicular brachial plexus block is a basic level block
Select a linear high-frequency probe. Adjust gain, focus and depth 3-4 cm
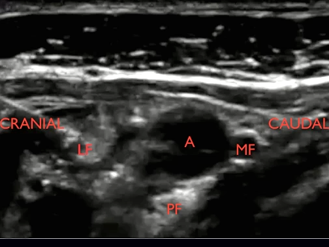
Turn the orientation mark on the probe cranially. Place the probe below the clavicle, medial to the coracoid process in the parasagittal plane
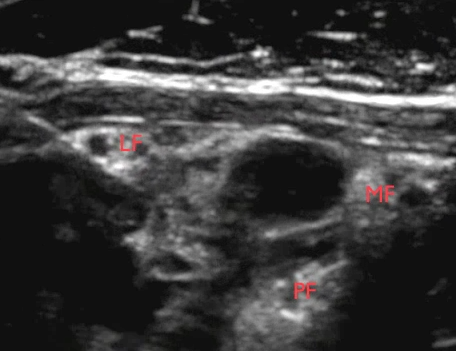
Locate the black, pulsatile axillary artery (AA) and align it to the centre of the monitor. Seeing AA as a clock face the lateral cord is located at nine o’clock, the posterior cord at six o’clock and the medial cord at two o’clock. Often the cords are not sonographically visible
Insert the needle below the clavicle and advance it in-plane aiming periarterially at seven o’clock. Empty the needle of air by injecting 1/2 mL local anaesthetic subcutaneously
Avoid piercing any vessels or nerves
The endpoint of injection is periarterially from two o’clock to ten o’clock. Reposition the needle tip as necessary to reach the endpoint

(B) Look for the axillary artery (A); lateral cord (L); medial cord (M); posterior cord (P). Anterior (ant), posterior (post)
In the infraclavicular block the local anaesthetic should be injected periarterially in the seven o’clock position (seeing the axillary artery as a clock face)
However, it is often necessary to reposition the needle tip in order to inject local anaesthetic periarterially from the two o’clock position around the artery to the ten o’clock position
Click on the VIDEO CLIP button to view the video
Repositioning of the needle tip is oftentimes necessary in order to cover all three cords around the axillary artery from two o’clock to ten o’clock
Care should be taken not to pierce the axillary vein
Click on the VIDEO CLIP button to view the video
In the video: Notice that local anaesthetic is injected on the wrong side of the clavipectoral fascia which has to be penetrated by the needle before local anaesthetic spreads appropriately around the medial cord
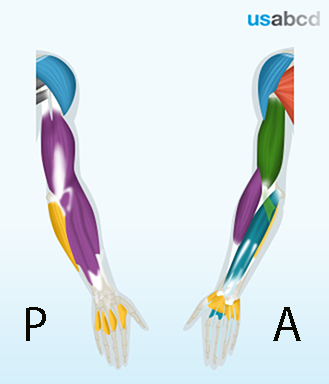
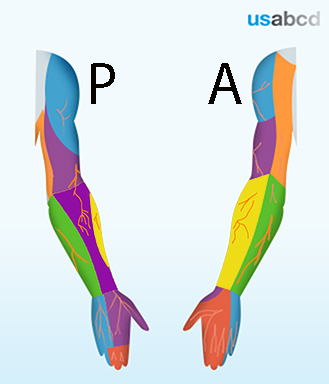
The infraclavicular brachial plexus block provides cutaneous anaesthesia of the entire upper limb
The radial nerve innervates the skin of the back of the brachium and the lateral hand
The musculocutaneous nerve innervates the skin of the lateral antebrachium
The ulnar nerve innervates the skin of the medial hand and fingers
The median nerve innervates the skin of the anterior part of the lateral hand and fingers and the distal dorsal part of the second and third finger
The skin of the medial arm and forearm is innervated by the medial cutaneous nerves of the arm and forearm. They are both derived from the medial cord of the brachial plexus and covered by the infraclavicular brachial plexus block
The radial nerve innervates the skin on the extensor side of the upper limb

The median nerve only innervates the skin on the hand

The cutaneous distribution of the ulnar nerve is only to the hand

The infraclavicular block anaesthetizes the brachial plexus inside the axilla
The brachial plexus in the infraclavicular region consists of three cords (syn: fascicles): the lateral, the posterior, and the medial cord
They run in close relationship to the axillary artery
That is exploited for the purpose of the infraclavicular brachial plexus block
The infraclavicular brachial plexus block covers all muscles of the upper limb distal to the shoulder:
The radial nerve innervates
– the elbow extensor muscles
– the wrist extensor muscles
The musculocutaneous nerve innervates the elbow flexor muscles
The ulnar nerve innervates the intrinsic muscles of the hand including the medial finger flexors
The median nerve innervates the wrist flexor muscles including the lateral finger flexors