Multiple B-lines can in some diseases be seen almost universally when scanning both lungs. This finding is often referred to as the interstitial syndrome (IS).
Multiple B-lines can in some diseases be seen almost universally when scanning both lungs. This finding is often referred to as the interstitial syndrome (IS).
As an example of a setting where focal B-lines still can be clinical useful, would be in a patient with clinical suspicion of pneumonia.
A lobar pneumonia with resulting increased density of the lobe, with corresponding B-lines would confirm the clinical suspicion.
If the density further increases and the lung tissue is filled with fluid and secretions the pattern will change to that of lung consolidation.
The finding of focal B-lines is not necessarily a sign of lung disease.
However, if used together with patient history and physical findings in clinical examination, the finding of focal B-lines may still be useful.

The occurrence of multiple, isolated B-lines can both be normal and a pathological sign.
In studies approx. 25% of patients with normal chest imaging have multiple B-lines in the lower lateral intercostal space.
The presence of focal areas with multiple B-lines can also be seen in any disease with a localised increased density of the lung tissue such as pneumonitis, atelectasis, pulmonary contusion, pulmonary embolism, pleural disease and malignancy.

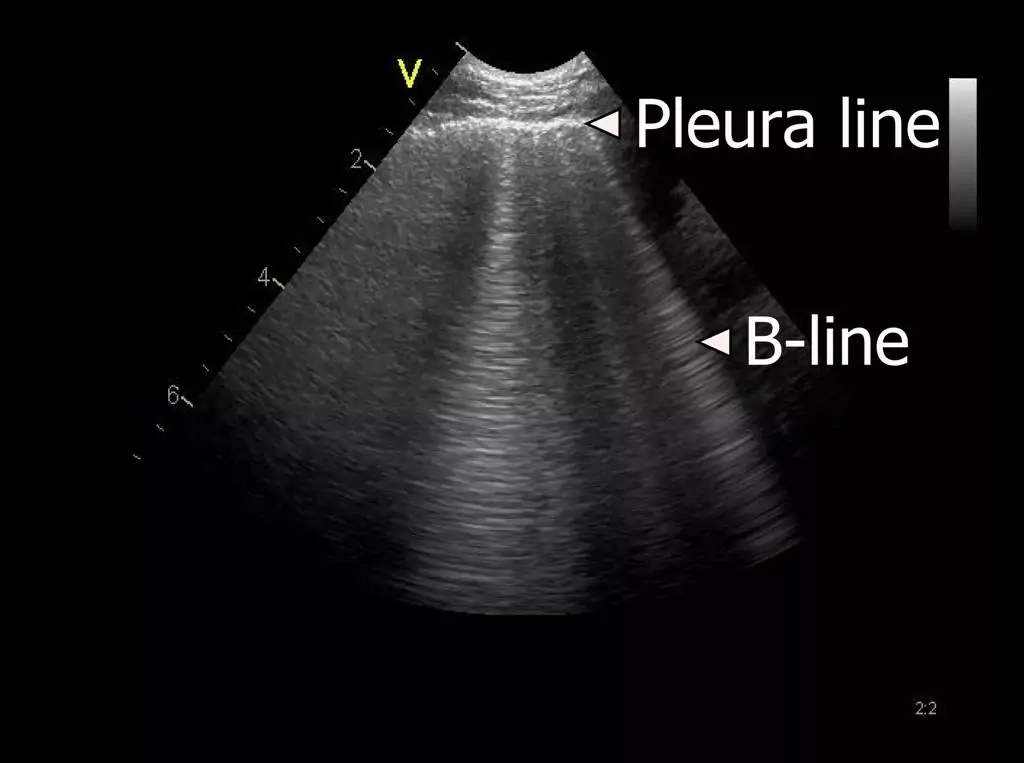
Other vertical hyperechoic artefacts may mimic the B-line, but these artefacts always become less hyperechoic or completely fades out.
In comparison, B-lines never fade out and can be visualised the entire way to the bottom of the field of view.

The presence of a characteristic artefact known as a B-line can be used as an indirect marker of lung disease.
B-line artefacts occur when the density of the lung has increased as for example in interstitial oedema or pulmonary fibrosis.
This lesson describes the B-line artifact and the interstitial syndrome (IS) in more detail.

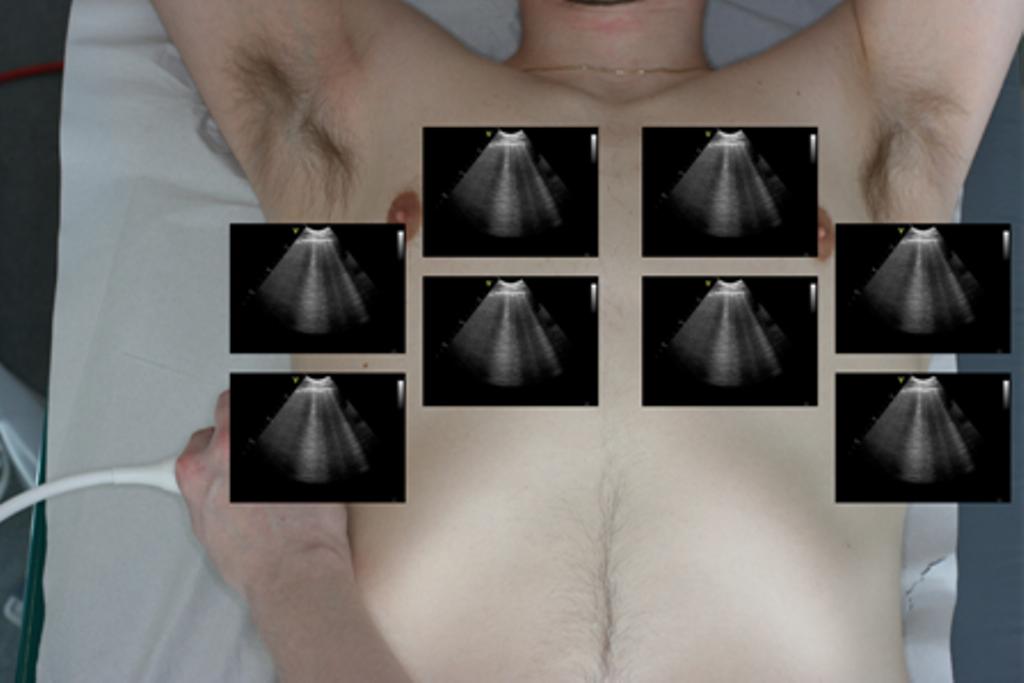
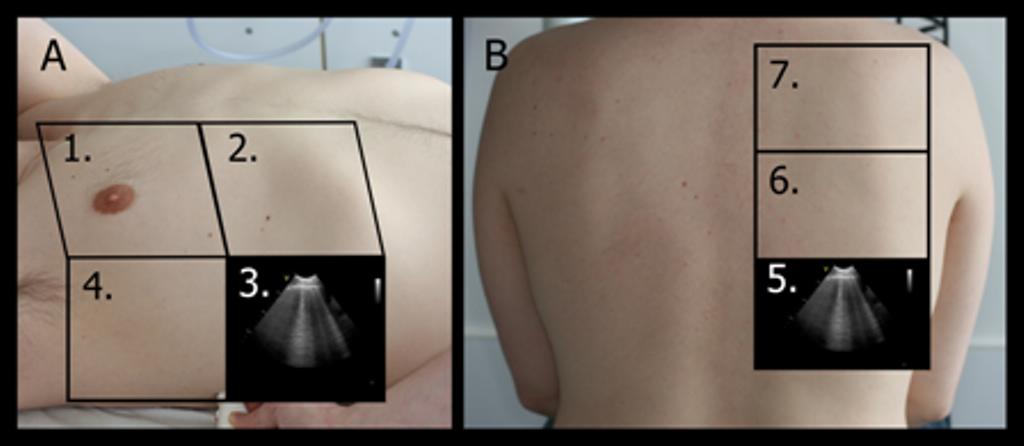
When performing FLUS, each hemithorax can be divided into an anterior, lateral and posterior surface, which can be further subdivided into smaller squares, representing a scanning zone, which should be assessed using FLUS*.
Each of the scanning zones can be denoted from 1R to 7R (R = right) and 1L to 7L (L = left).

In order to save time, the two lateral transducer positions used for the evaluation of possible pleural effusion can easily be integrated with the transducer placement used for the evaluation of the hepatorenal fossa and splenorenal fossa normally performed as a part of a FAST examination.

Four positions for transducer placement are used for the thoracic evaluation in E-FAST.
Two anterior positions are used for the evaluation of pneumothorax and two lateral positions are used for the evaluation of pleural effusion.
Anterior positions:
– Right hemithorax: 2. Intercostal space in the medioclavicular line
– Left hemithorax: 2. Intercostal space in the medioclavicular line
Lateral positions:
– Right hemithorax: 4. Intercostal space in the posterior axillary line
– Left hemithorax: 4. Intercostal space in the posterior axillary line

