At the infero-lateral margin of the minor pectoral muscle the strong Gerdy’s ligament (= the lower part of the clavicopectoral fascia) connects the minor pectoral muscle to the axillary fascia
When the needle tip penetrates Gerdy’s ligament it enters the the lower part of the axillary space between the Gerdy’s ligament antero-laterally and the serratus anterior muscle covering the lateral thoracic wall medially in the axilla
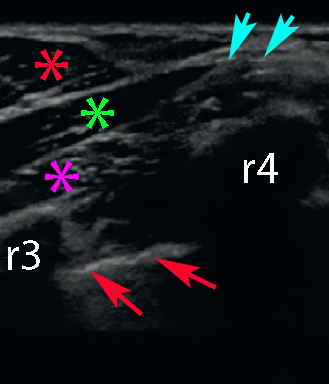
Gerdy’s ligament (cyan arrows), minor pectoral muscle (green asterix), major pectoral muscle (red asterix), serratus anterior (magenta asterix), pleura (red arrows), ribs III and IV (r3 and r4)
The needle is inserted in-plane from the cranial end of the probe until the tip of the needle penetrates the infero-lateral margin of the minor pectoral muscle and enters the lower part of the axilla between the Gerdy’s ligament and the serratus anterior muscle
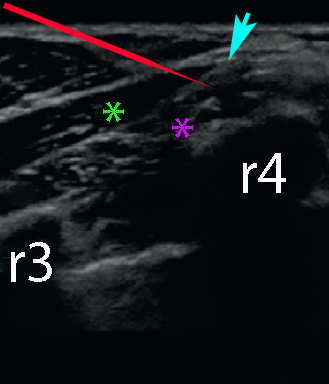
Gerdy’s ligament (cyan arrow), minor pectoral muscle (green asterix), serrratus anterior muscle (magenta asterix), needle (red), rib III (r3), rib IV (r4)
Blanco R: The ‘pecs block’: a novel technique for providing analgesia after breast surgery. Anaesthesia 66(9): 847–848 (2011)
Blanco R, Fajardo M, Parras Maldonado T: Ultrasound description of Pecs II (modified Pecs I): A novel approach to breast surgery. Rev Esp Anestesiol Reanim. (2012) (http://dx.doi.org/10.1016/j.redar.2012.07.003)
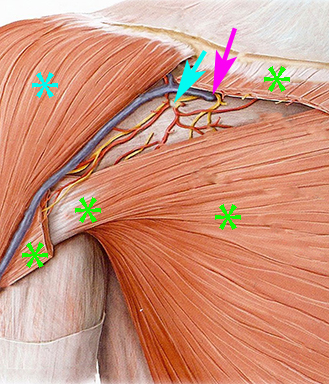
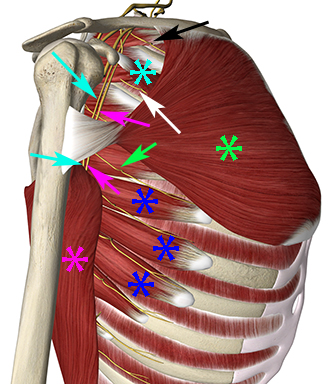
The part of the clavipectoral fascia close to the clavicle – the costocoracoid ligament – is penetrated by the cephalic vein, the lateral pectoral nerve and the thoracoacromial artery
The clavipectoral fascia is pierced by the lateral pectoral nerve together with the cephalic vein (magenta arrow) and by the thoracoacromial artery (cyan arrow). The cephalic vein runs upward in the deltopectoral groove between the deltoid muscle (cyan asterix) and the major pectoral muscle (green asterisks)
The anterior wall of the axilla consists of the major and minor pectoral muscles and the clavipectoral fascia
The medial wall of the axilla is the lateral thoracic wall with costae I-IV and intercostal muscles – and the serratus anterior muscle
The lateral wall is the intertubercular groove of the humerus and the posterior wall is the subscapularis, teres major and latissimus dorsi muscles.
The axilla contains some nerves that are relevant for axillary extension of breast surgery:
1) the lateral cutaneous branches of the intercostal nerves 2) the anterior intercostal branches of the intercostal nerves 3) the long thoracic nerve that innervates the serratus anterior muscle 4) the thoracodorsal nerve that innervates the latissimus dorsi muscle
Lateral cutaneous branch of intercostal nerves I (black arrow), II (white arrow), IV (green arrow), major and minor pectoral muscles (green and cyan asterixs), latissimus dorsi (magenta asterix), serratus anterior (blue asterix), long thoracic nerve (magenta arrows), thoracodorsal nerve (cyan arrows)
The intercostal nerves run in the intercostal spaces sandwiched between the socalled innermost intercostal muscle and the internal and external intercostal muscles superficially joined by the intercostal arteries and veins
The lateral cutaneous branches of the intercostal nerves branch off in the midaxillary line, pierce the internal and external intercostal muscles and branch into a posterior and an anterior terminal branch; the latter runs anterior to innervate the skin covering the infero-lateral part of the breast
The anterior cutaneous branches of the intercostal nerves run anterior to the internal mammary artery, pierce the intercostal membranes and innervate the medial part of the breast
The lateral cutaneous branches (syn: lateral mammary branches) of the intercostal nerves innervate the skin of the axilla (the intercostobrachial nerve, which is the lateral cutaneous branch from intercostal nerve T2 innervates part of the skin of the axilla and continues to innervate the skin of the proximal medial surface of the arm) and the lateral part of the breast
The anterior cutaneous branches (syn: medial cutaneous branches or medial mammary branches) of the intercostal nerves innervate the supero-medial part of the breast
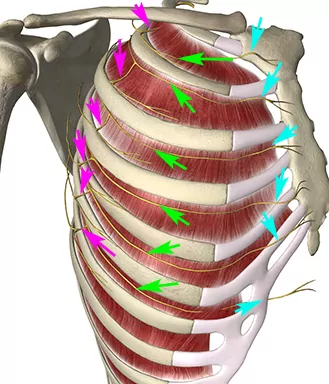
Lateral cutaneous branches of the intercostal nerves (blue arrows and purple area).
Anterior cutaneous branches of the intercostal nerves (magenta arrows and red area)
Place the probe in the sagittal plane below the lateral third of the clavicle and identify the axillary artery and vein below the pectoral muscles
Rotate the probe to obtain an oblique orientation with the proximal end of the probe medial and the distal end of the probe lateral
Visualize the sonoanatomical target (see next pages)
Insert the needle with in-plane technique from the proximal end of the probe and advance the needle tip to the target (see next pages) before injecting the local anaesthetic
Inject 10 mL for the PECS I block and step one of the PECS II block. Inject a supplementary 20 mL for step two of the PECS II block
Start by placing the probe sagittal (se picture) and then rotate the probe to an oblique orientation
The local anaesthetic is injected into the fascial space between the muscle fascia of the major pectoral muscle anteriorly and the clavipectoral fascia with the minor pectoral muscle posteriorly
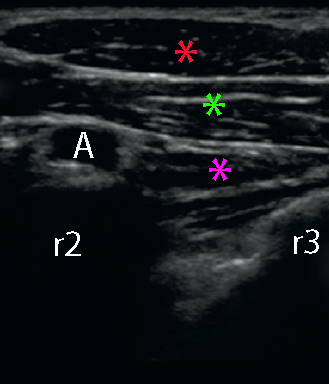
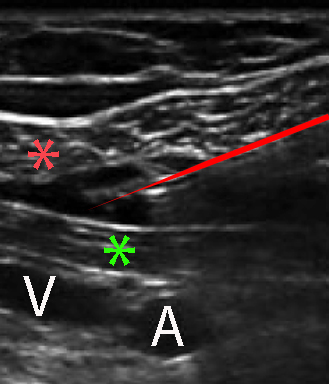
Major pectoral muscle (red asterix), minor pectoral muscle (green asterix), red needle, axillary artery (A), axillary vein (V).
The black expansion between the major and minor pectoral muscles around the tip of the needle is the local anaesthetic