The Bilateral Dual TAP block (BD-TAP block) is a combination of four TAP blocks
Together the four blocks anesthetise the entire antero-lateral abdominal wall including the parietal peritoneum – but excluding the visceral peritoneum: Bilateral intercostal TAP block combined with bilateral classic TAP block
The indications for the BD-TAP block are:
– Perioperative pain management for abdominal surgery
– Post-operative rescue pain management after abdominal surgery
Laparoscopic abdominal surgery indicates a BD-TAP block
The anterior rami of spinal nerves Th6 to L1 innervate the antero-lateral abdominal wall. They include the intercostal (Th6-Th11), the subcostal (Th12), and the iliohypogastric/ilioinguinal nerves (L1)
These nerves give rise to lateral cutaneous branches in the neurovascular plane called the transversus abdominis plane (TAP) between the internal oblique and the transversus abdominis muscles
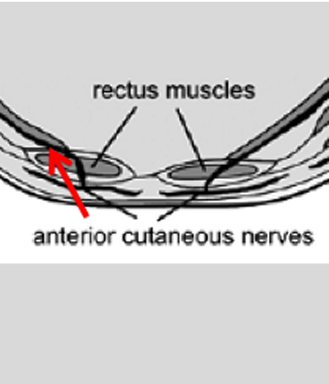
Th6-Th12 pierce the rectus sheath and end as anterior cutaneous nerves. They provide sensory innervation to the skin, costal parts of diaphragm, related parietal pleura and the parietal peritoneum
Th6-7 give sensory innervation at the epigastrium, Th10 at the umbilicus, and L1 at the groin
Th6-L1 contribute motor innervation to overlying oblique muscles, the transversus abdominus muscle, the pyramidalis and the rectus abdominis muscle
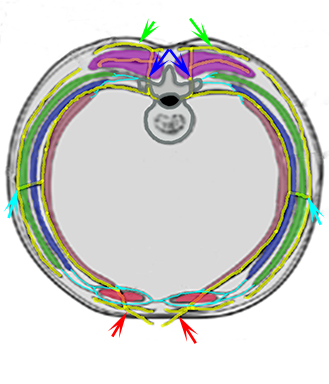
The anterior spinal rami (yellow): anterior, lateral and dorsal cutaneous branches (red, cyan and green arrows), dorsal branches (blue arrows), external (green) and internal (blue) abdominal muscles, transverse abdominal muscle (brown), rectus abdominis (red), intrinsic back muscles (purple), rectus sheath (cyan)
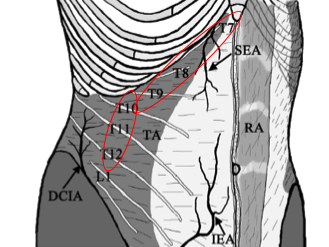
All thoracolumbar nerves that innervate the anterior abdominal wall travel as multiple mixed segmental nerves, which branch and communicate widely within the transversus abdominis plane (TAP) (1) anterolaterally (intercostal TAP plexus = Th6-Th9) (2) in plexuses that run with the deep circumflex iliac artery (DCIA) (classical TAP plexus = Th10-Th12) and (3) the deep inferior epigastric artery (DIEA) (rectus sheath plexus)
Segmental nerves Th6 to Th9 emerge from the costal margin to enter the TAP between the midline and the anterior axillary line
Th6 enters the TAP just lateral to the linea alba
Th7-Th9 emerge from the costal margin at increasingly lateral positions
Branches of Th9 emerge from the costal margin either medial or lateral to the anterior axillary line
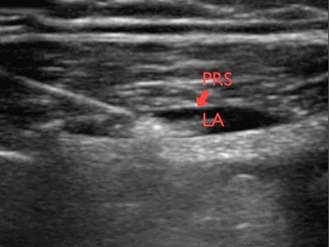
When anaesthetising the upper abdomen (above the umbilicus), the local anaesthetic must be positioned as high and medial as possible
This means behind the posterior rectus sheath (and rectus abdominis muscle) and above the transversus abdominis muscle. This is called the intercostal TAP block
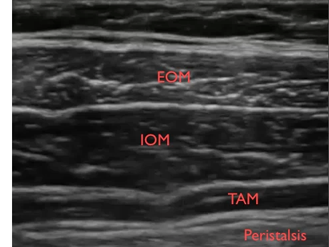
When anaesthetising the lower abdomen (below the umbilicus), the needle entry point must be above the iliac crest and below the thoracic cage with the insertion point being in the anterior axillary line
The local anaesthetic must be positioned in the neurovascuar plane between the internal oblique and transversus abdomens muscles