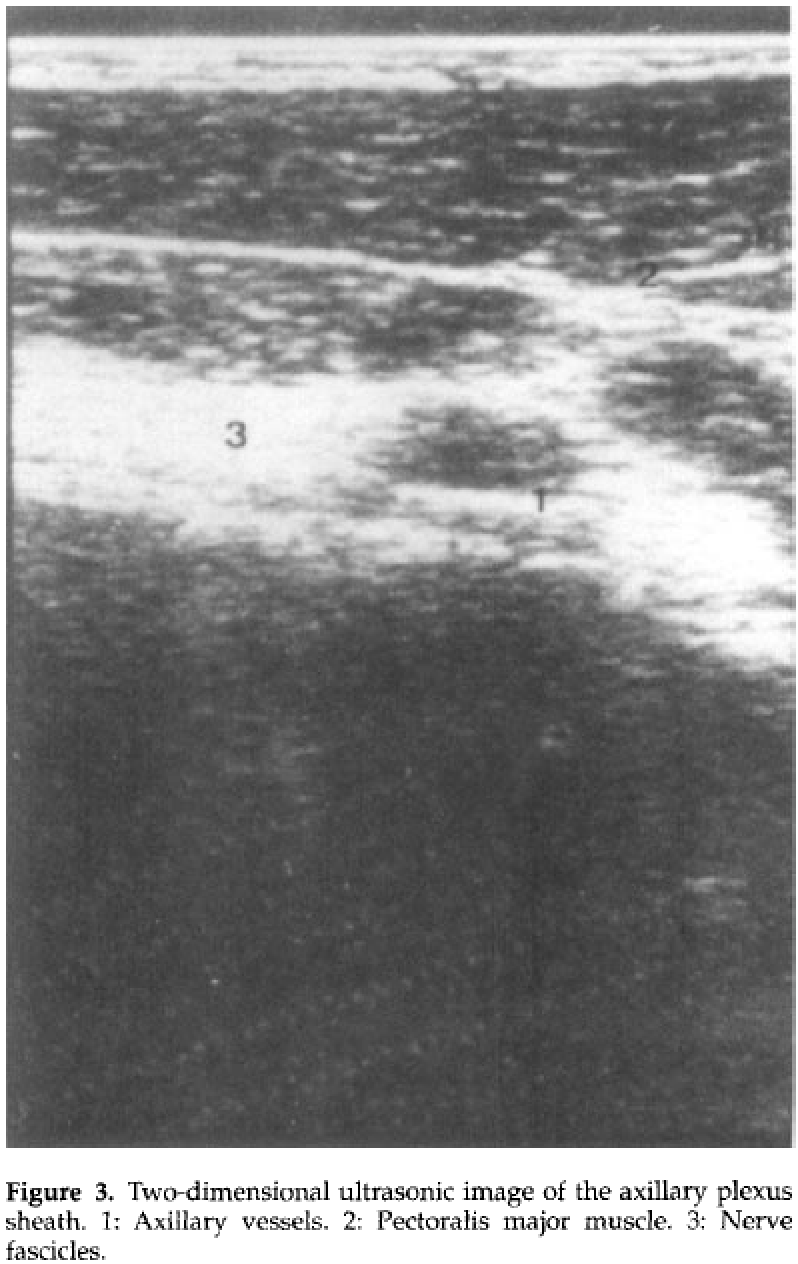
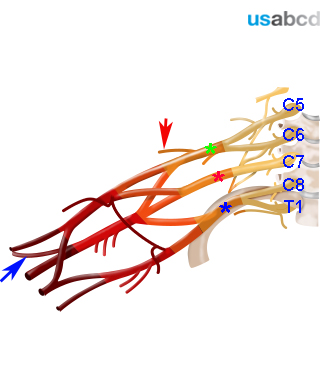
The brachial plexus runs across the first rib in close relationship to the subclavian artery
On top of the first rib the branches of the brachial plexus are located postero-superior to the artery
The brachial plexus runs across the first rib in close relationship to the subclavian artery
On top of the first rib the branches of the brachial plexus are located postero-superior to the artery
Align the pulsatile subclavian artery to the center of the monitor
Rotate and tilt the transducer to obtain the best possible SAX view of the pulsatile subclavian artery and brachial plexus nerve divisions
Adjust depth, gain and focus
The hyperechoic first rib has to be exactly underneath the vessel. The pleura is posterior to the first rib. (Note air artifact, periodic “comet tail” sign and lung sliding movement in the pleural space)
The nerve divisions of the brachial plexus are a hyperechoic cluster lateral and posterior to the artery – they are round and dark with a bright rim
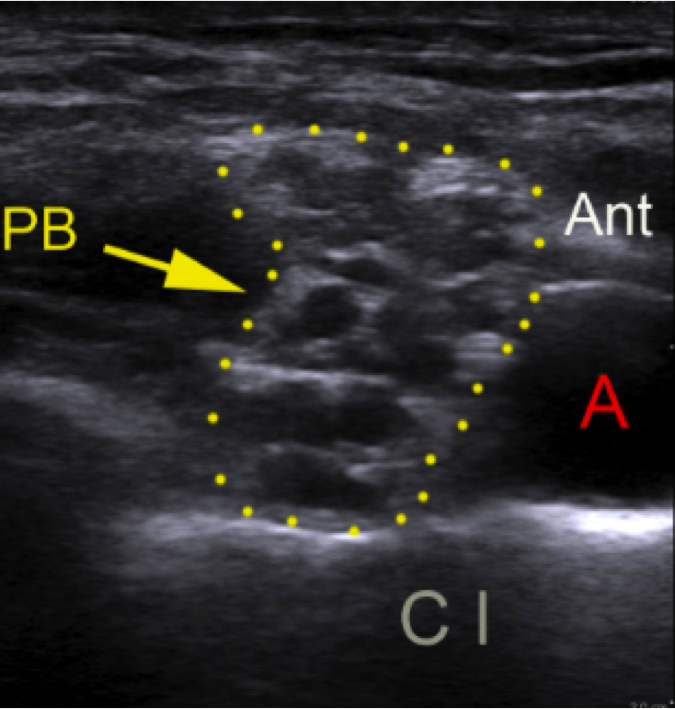
The lowermost branches of the brachial plexus – originating from the C8 and T1 spinal nerve roots – run across the first rib in the corner between the rib and the subclavian artery
This is called the corner pocket
It is important to locate the probe on top of the first rib
With in-plane needle approach the needle tip will impinge on the rib instead of producing a pneumothorax, if the needle is inserted too deep
Local anesthetic has to be injected in the angle between the subclavian artery, the first rib and the bundle of nerve divisions
SA = subclavian artery
nd = bundle of nerve divisions
p = pleura
c1 = first rib
It is mandatory to insert the needle with in-plane technique for the supraclavicular brachial plexus block in order to minimize the risk of pneumothorax
The supraclavicular brachial plexus block is indicated for surgical anaesthesia and postoperative analgesia for procedures of the upper limb distal to the shoulder level

The supraclavicular brachial plexus block targets the brachial plexus at the level of the zone of transition – where the trunks are transformed to fascicles just proximal to the clavicle
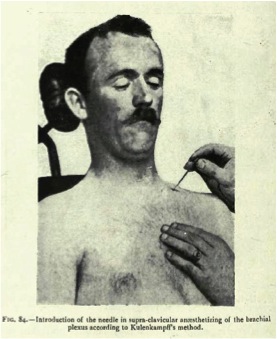
The first transcutaneous, supraclavicular brachial plexus block in history was performed approximately 100 years ago – in 1911 – by the German surgeon Dietrich Kulenkampf
Ever since anaesthesiologists have performed transcutaneus, peripheral nerve blocks blindfolded until the emergence of ultrasound guided nerve blocks introduced by Stephan Kapral in 1996
Dietrich Kulenkampf published his technique in “Zur anästhesierung der Plexus Brachialis”, Zentralblatt für Chirurgie, 38:1337-1340 (1911)
Stephan Kapral from Vienna was the first who presented an US guided nerve block with real-time visualisation of the target nerves and the perineural spread of local anaesthetic
It was a supraclavicular brachial plexus block
Kapral S, Kraff P, Eibenberger K, Fitzgerald R, Gosh M, Weinstabl C: Ultrasound-guided supraclavicular approach for regional anesthesia of the brachial plexus. Anesthesia & Analgesia, 78:507-513 (1994)