The rectus sheath is made by the anterior aponeuroses of the lateral abdominal muscles (external and internal obliques and the transverse abdominis) that split into an anterior and a posterior layer that encloses the rectus abdominis muscle on each side; the two layers fuse on the medial side of the rectus muscle and attach to the linea alba
The anterior layer of the rectus sheath extends from the xiphoid process to the pubic symphysis
The posterior layer only extends 3-5 cm below the umbilicus to the socalled arcuate line and it is separated from the peritoneum by the transversalis fascia
The 9th, 10th, and 11th intercostal nerves and the epigastric blood vessels are sandwiched between the rectus abdominis muscle fascia and the posterior layer of the rectus sheath
Blockade of these nerves with a rectus sheath block produces periumbilical anaesthesia
Rectus abdominis muscles (red asterixs), posterior rectus muscle fascia (red arrow), posterior layer of the rectus sheath (green arrows), aponeuroses of the lateral abdominal muscles (black arrows), linea alba (magenta arrow), fascia transversalis (blue arrows), parietal peritoneum (cyan arrows)
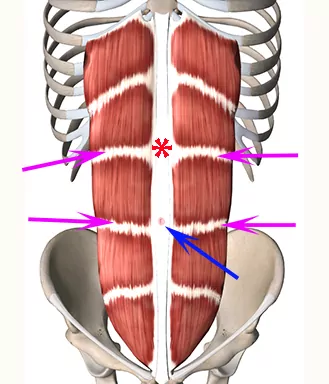
The tendinous inscriptions of the rectus abdominis muscle are not attached to the posterior lamina of the rectus sheath
This means that local anaesthetic injected between the rectus abdominis muscle and the posterior lamina in theory can spread along the backside of the rectus abdominis muscle and anaesthetize the anterior cutaneous branches of the 9th, 10th and 11th intercostal nerves
Rectus abdominis muscle with tendinous inscriptions (magenta arrows), umbilicus (blue arrow), and linea alba (red asterix)
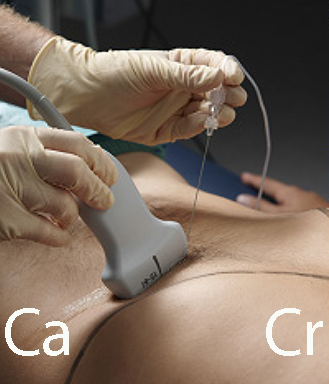
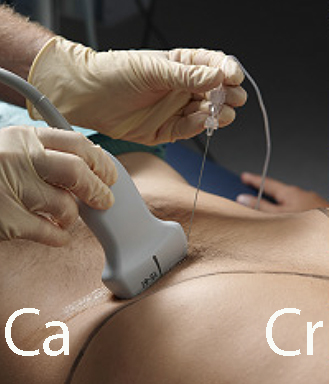
– Place the high-frequency linear probe with the medial end just on top of the linea alba
– Visualize the linea alba, the rectus abdominis, and the posterior rectus sheath (see next page)
– Use color Doppler to identify the epigastric arteries
– Advance the needle through the rectus abdominis muscle until the needle tip enters the space between the belly of the muscle and the posterior layer of the rectus sheath
– Inject 10 mL of local anaesthetic per side in adults. In children 0.5 mg ropivacaine/kg can be injected per side
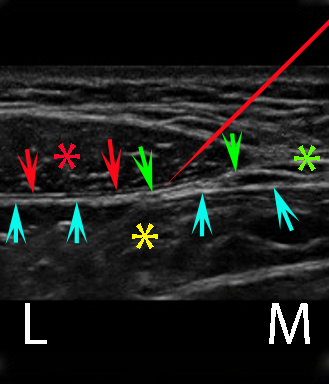
The needle is advanced to the fascial plane between the muscle fascia of the rectus abdominis and the posterior layer of the rectus sheath (see picture)
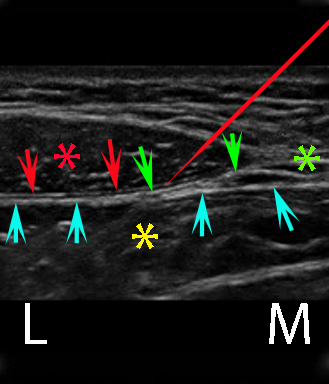
Rectus abdominis (red asterix), rectus abdominis muscle fascia (red arrows), linea alba (green asterix), posterior layer of the rectus sheath (green arrows), peritoneal cavity (yellow asterix), parietal peritoneum and transversalis fascia (cyan arrows), needle (red). L = lateral, M = medial.