The advantage of the in-plane approach to block the femoral nerve is that the target nerve and the needle tip and the spread of the injected local anaesthetic can be observed simultaneously
Click on the VIDEO CLIP button to view the video
The advantage of the in-plane approach to block the femoral nerve is that the target nerve and the needle tip and the spread of the injected local anaesthetic can be observed simultaneously
Click on the VIDEO CLIP button to view the video
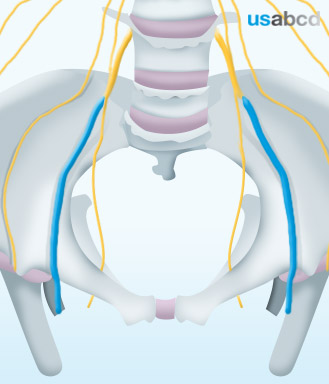
The lumbar part of the lumbosacral plexus emerges from five spinal nerves: T12, L1, L2, L3 and L4
It gives origin to three important nerves in lower limb innervation: The femoral, the obturator and the lateral femoral cutaneous nerves
The most important lumbar plexus nerve concerning basic peripheral nerve blockade is the femoral nerve
It originates from the L2, L3, and L4 spinal nerves of the lumbar plexus
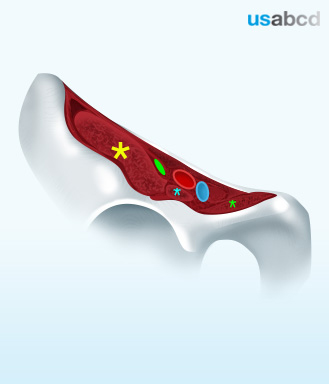
In the inguinal region the femoral nerve (FN) runs lateral to the femoral vessels and on top of the iliopsoas muscle
The femoral nerve runs below the iliacus fascia
To reach the nerve with your needle you have to penetrate two fascia: fascia lata and the iliacus fascia
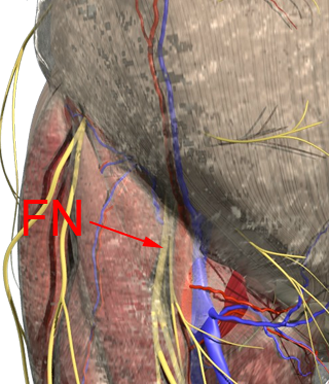
The femoral nerve runs below the iliacus fascia and on top of the iliacus muscle
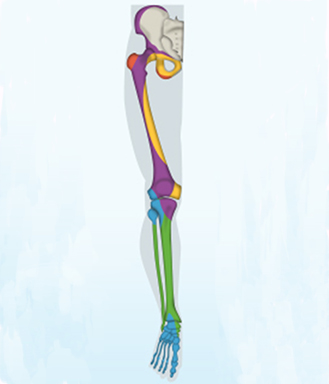
The branches of the femoral nerve innervate the anterior side of:
– the hip joint
– the femoral bone
– the knee joint including the patella
– the medial tibial epicondyle
A femoral branch to the hip joint arises from the nerve to rectus femoris
Branches to the knee joint arise from each of the nerves supplying the vastus muscles with a fourth branch from the saphenous nerve
The femoral nerve splits into the anterior and the posterior branch
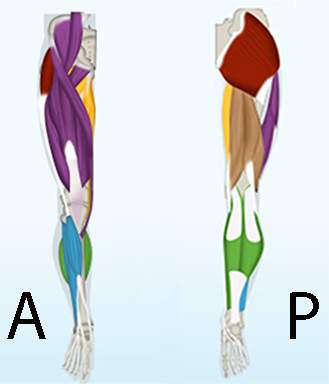
The femoral nerve innervates the muscles in the anterior compartment of the thigh
The anterior branch of the femoral nerve innervates the sartorius muscle – and sometimes the pectineus muscle
The posterior femoral nerve branch innervates most of the muscles in the anterior compartment of the thigh – i.e. the quadriceps femoris (the rectus femoris and the three vastus muscles)
Before the femoral nerve emerges from under the inguinal ligament it also innervates the iliac muscle and the femoral artery
Position: place the patient supine, rotate the thigh external
Probe: select a linear, high-frequency transducer
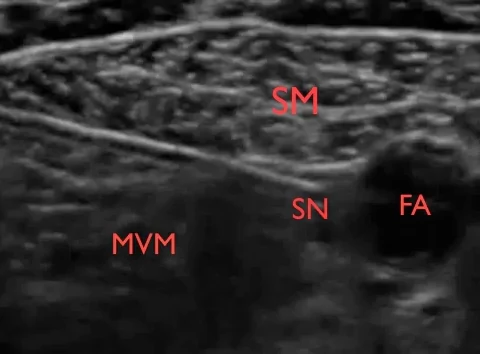
Place/Plane: place the transducer mid-thigh medially and perpendicular to the adductor canal
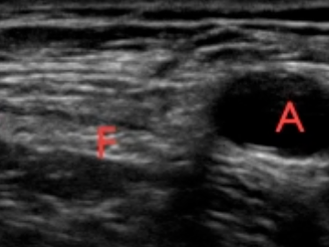
First locate the pulsatile femoral artery
You may track the artery from the inguinal ligament until it dives under the sartorius muscle

Local anaesthetic is injected just lateral to the femoral artery in the triangular space between the femoral artery, the sartorius muscle and the medial vastus muscle
Click on the VIDEO CLIP button to view the video
The saphenous nerve is a branch of the posterior branch of the femoral nerve
The saphenous nerve innervates the antero-medial part of the knee and the leg including the medial malleolus and and the anterior side of the ankle joint and the subtalar joints

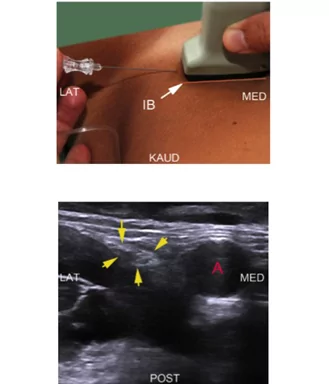
– Place a linear high-frequency probe in the inguinal groove and identify the pulsatile femoral artery
– Align the artery to the centre of the monitor by adjusting the position of the probe and the depth of the image
– Locate the femoral nerve (FN) lateral to the artery on top of the iliac muscle. The FN is usually flattened, spindle-shaped or triangular – rarely round
– Capture the best possible cross-sectional image of the FN by tilting the probe 10-30 degrees cranially
– Insert the needle from the lateral end of the probe
– Advance the needle inside the plane of the ultrasound beam (in-plane, IP) until the tip of the needle touches the deep surface of the FN tangentially
– The endpoint is complete perineural spread of local anaesthetic