In patients who have been admitted for a while in an intensive care unit (ICU), many diseases and conditions may cause interstitial syndrome
Hence, LUS with signs of interstitial syndrome, is a less specific finding in this setting
In patients with acute respiratory failure to an intensive care unit, the finding of interstitial syndrome is however most often due to cardiogenic pulmonary edema
Despite these limitations FLUS can still as an efficient tool to rule-out these conditions
Supplementary use of other kinds of point-of-care sonography such as focus assessed transthoracic echocardiography (FATE) can be of further use to differentiate between cardiogenic and non-cardiogenic causes of interstitial syndrome
FLUS video from a patient with acute respiratory failure
Since no B-lines were present, IS was absent and pulmonary edema could be ruled-out
The finding of interstitial syndrome is a powerful diagnostic tool in diagnosis of pulmonary edema
FLUS is very sensitive for detecting interstitial oedema. Consequently, a FLUS examination with no signs of interstitial syndrome can be used to rule out conditions such as cardiogenic pulmonary oedema
FLUS from zone 3R in a patient with cardiogenic pulmonary edema. Multiple B-lines and a small pleural effusion are present
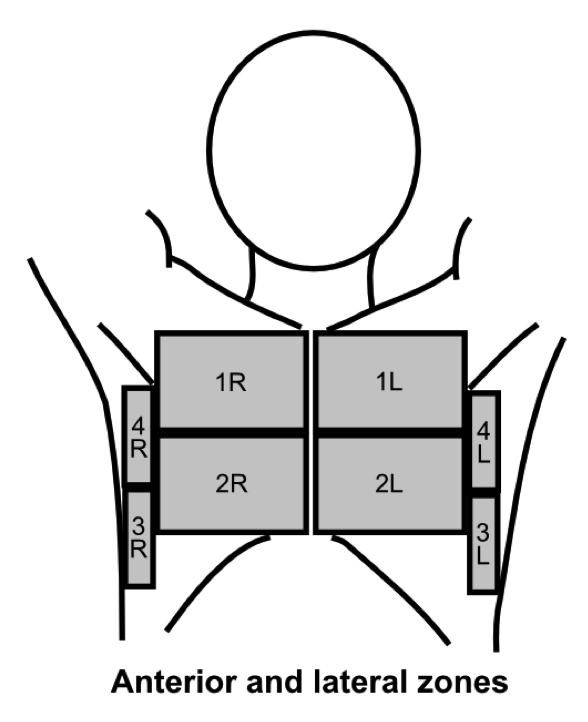
Using the scanning technique described in the examination technique module, with two anterior, two lateral and three posterior scanning zones, the criteria for IS is the presence of both of the following:*
1: A positive scanning zone is defined by the presence of three or more B-lines in a longitudinal plane between two ribs
2: When scanning the anterior and lateral zones, two or more of the zones have to be positive on each side
* Volpicelli, G., et al., “International evidence-based recommendations for point-of-care lung ultrasound”, Intensive Care Med, 2012, 38(4): p. 577-91
The image depicts the anterior and lateral zones used for the assessment of interstitial syndrome
Multiple B-lines can in some diseases be seen almost universally when scanning both lungs. This finding is often referred to as the interstitial syndrome (IS)
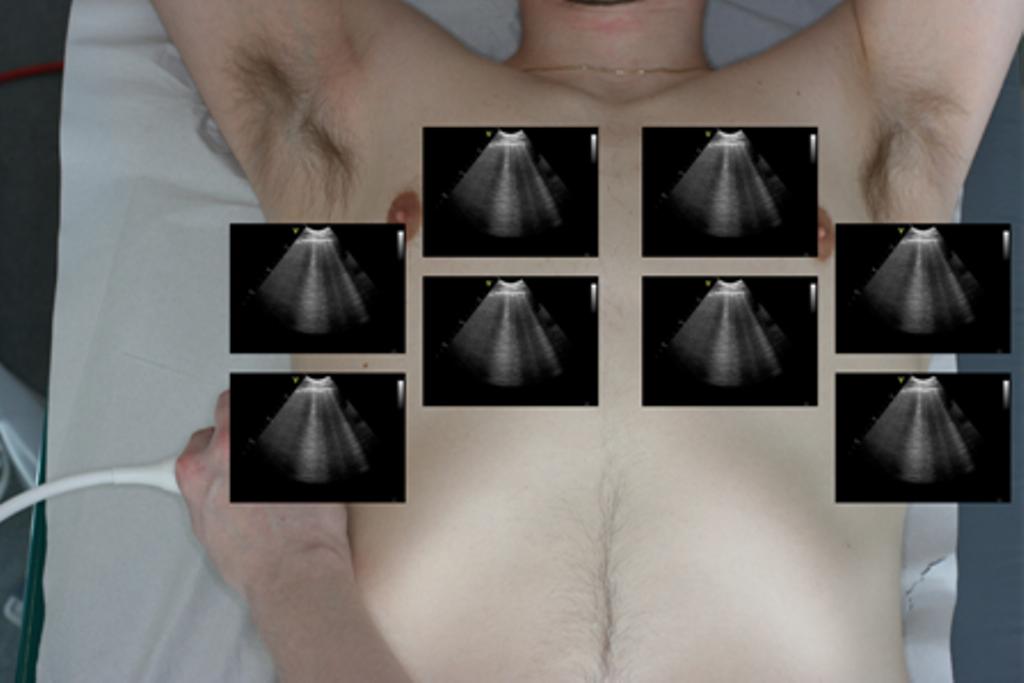
FLUS findings in a patient with multiple B-lines in all anterior and lateral zones bilaterally
The occurrence of multiple, isolated B-lines can both be normal and a pathological sign
In studies approx. 25% of patients with normal chest imaging have multiple B-lines in the lower lateral intercostal space
The presence of focal areas with multiple B-lines can also be seen in any disease with a localised increased density of the lung tissue such as pneumonitis, atelectasis, pulmonary contusion, pulmonary embolism, pleural disease and malignancy
When assessing zone 3, multiple B-lines in the lower lateral intercostal space can be a normal finding