• Abdominal or pelvic surgeries for cancer
• Major trauma
• Craniotomy/spinal surgery for malignant disease
• Spinal surgery with anterior approach
• Thoracic surgeries
• Major orthopedic surgery
Reference:
Heit JA, Melton LJ, Lohse CM, et al. Incidence of venous thromboembolism in hospitalized patients versus community residents. Mayo Clin Proc 2001; 76: 1102-10.
Symptomatic perioperative venous thromboembolism is a frequent complication in patients with a history of deep vein thrombosis (1).
Incidence of DVT in perioperative population:
3.6% of patients presenting for percutaneous kyphoplasty (2)
6.4% of patients with ankle fractures (3)
3.7% of patients with lower extremity fractures, and 6.2% of post-operative patients (4)
4.4% of patients presenting for gastric cancer surgery, and 7.2% of post-operative gastric cancer patients (5)
Venous thromboembolism is a factor in 5% of patients that die within 30 days postoperatively (6)
References:
1) Liem TK, Huynh TM, Moseley SE, Minjarez RC, Landry GJ, Mitchell EL, Deloughery TG, Moneta GL. Symptomatic perioperative venous thromboembolism is a frequent complication in patients with a history of deep vein thrombosis. J Vasc Surg. 2010 Sep; 52(3): 651-7.
2) Fan, Wencan MDa; Qiao, Tianzhu MDa; You, Yongqing MDb,?; Zhang, Jun MDc; Gao, Jijian MDd,? Perioperative prevalence of deep vein thrombosis in patients with percutaneous kyphoplasty, Medicine: March 2020 – Volume 99 – Issue 10 – p e19402.
3) Luo, Z., Chen, W., Li, Y. et al. Preoperative incidence and locations of deep venous thrombosis (DVT) of lower extremity following ankle fractures. Sci Rep 10, 10266 (2020).
4) Wang H, Kandemir U, Liu P, Zhang H, Wang PF, Zhang BF, Shang K, Fu YH, Ke C, Zhuang Y, Wei X, Li Z, Zhang K. Perioperative incidence and locations of deep vein thrombosis following specific isolated lower extremity fractures. Injury. 2018 Jul; 49(7): 1353-1357.
5) Osaki T, Saito H, Fukumoto Y, Kono Y, Murakami Y, Shishido Y, Kuroda H, Matsunaga T, Sato K, Hirooka Y, Fujiwara Y. Risk and incidence of perioperative deep vein thrombosis in patients undergoing gastric cancer surgery. Surg Today. 2018 May; 48(5): 525-533.
6) The Vascular Events in Noncardiac Surgery Patients Cohort Evaluation (VISION) Study Investigators. CMAJ July 29, 2019 191 (30) E830-E837.
VTE is a leading cause of preventable hospital death in the USA.
VTE is the fifth most frequent reason for unplanned hospital readmissions after surgery, overall.
Blood clots affect as many as 900,000 Americans each year leading to approximately 100,000 premature deaths.
References:
• Society of Hospital Medicine, Maynard GA, Stein JM, US Agency for Healthcare Research and Quality. Preventing hospital-acquired venous thromboembolism: a guide for effective quality improvement. Rockville, MD: Agency for Healthcare Research and Quality, US Dept. of Health and Human Services; 2008.
• Spencer F, Lessard D, Emery C, Reed G, Goldberg R. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007; 167(14): 1471-5.
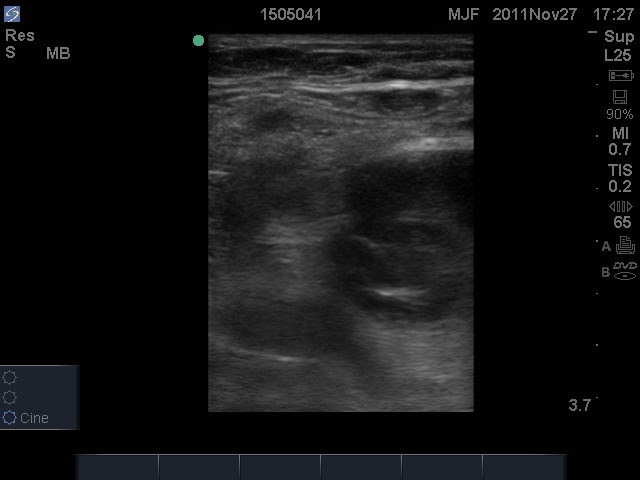
Point of care ultrasound can determine the presence of deep venous thrombosis (DVT) in the lower extremity of patients in critical situations.
DVT evaluation may be useful for anesthesiologists, emergency physicians, or intensivists, or other physicians. There is utility of DVT evaluation in clinics, emergency departments, preoperative evaluation, post-operative period, or when patients are in critical condition
Authors of the e-learning program:
William Manson, MDJan Boublik, MD PhDStephen Haskins, MD
The evaluation of deep venous thrombosis (DVT) shares the following characteristics with other point-of-care ultrasound applications:
• It is performed by clinicians treating the patient at the bedside or at the “point of care.”
• It answers a clear diagnostic question that guides clinical care and immediately improve patient outcomes.
• The exam is focused and goal directed, limited in scope, and answers a binary question.
• The findings are easy to recognize.
• The exam is easily learned and quickly performed.
The evaluation of deep venous thrombosis (DVT) shares the following characteristics with other point-of-care ultrasound (PoCUS) applications:
• It is performed by clinicians treating the patient at the bedside or at the “point of care.”
• It answers a clear diagnostic question that guides clinical care and immediately improve patient outcomes.
• The exam is focused and goal directed, limited in scope, and answers a binary question.
• The findings are easy to recognize.
• The exam is easily learned and quickly performed.