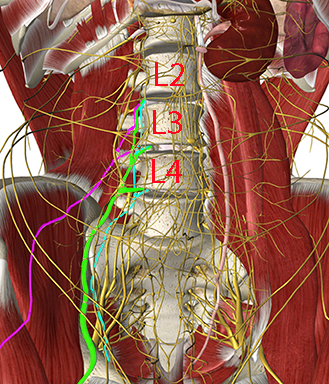
The important target nerves for the lumbar plexus block are the femoral nerve (L2-L4), the obturator nerve (L2-L4), and the lateral femoral cutaneous nerve (L2-L3)
The other lumbar plexus nerves are not targeted with the lumbar plexus block, but are blocked selectively for some purposes (see other modules in this learning program): The iliohypogastric nerve (T12-L1), the ilioinguinal nerve (L1) and the genitofemoral nerve (L1-L2)
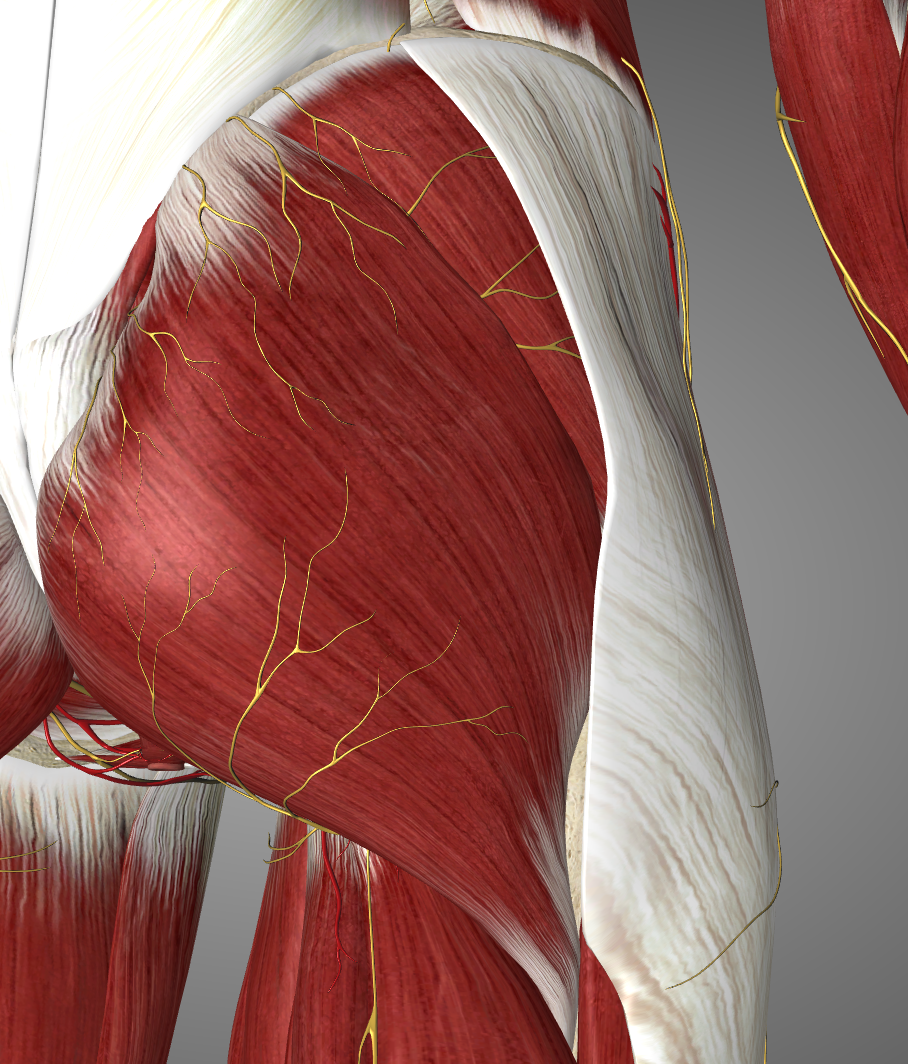
The femoral nerve innervates the iliopsoas, pectineus, sartorius, and quadriceps femoris muscles. It supplies sensory innervation to the hip joint, the anterior cutaneous branches of the thigh, the knee joint and via the saphenous nerve sensory branches to the knee region, the medial leg including branches to the medial ankle and subtalar joint capsules
The obturator nerve innervates the adductors (longus, brevis, magnus), gracilis, pectineus, and obturator externus
The lateral femoral cutaneous nerve supply sensory innervation to the lateral thigh
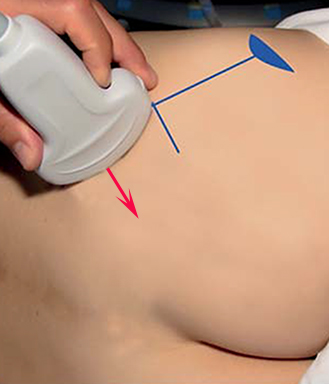
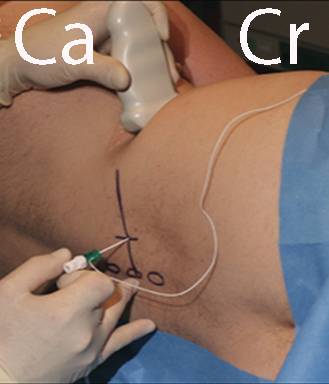
Place the patient in the lateral decubitus position
Place a low-frequency curved array probe in the axial plane in the flank just cranial to the iliac crest
The muscles of the abdominal wall are visualized (see next page). The probe is moved dorsal until the quadratus lumborum is seen medial to the aponeurosis of the transversus abdominis
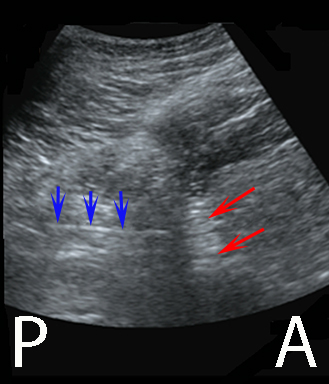
With a slight caudal tilt of the probe, the body and transverse process (TP) of vertebral body L4 can be seen surrounded by the “shamrock muscles” (see next page)
The lumbar plexus is visualized anterior to the TP (see second next page)
The needle is inserted from the back of the patient with in-plane technique and the needle tip is guided by ultrasound and electrical nerve stimulation to the target lumbar plexus (see third next page). Inject 20-30 mL of local anaesthetic.
The ultrasound guided “shamrock” lumbar plexus block
The muscles of the abdominal wall (external and internal obliques and transversus abdominis) are visualized
The probe is moved dorsal until the quadratus lumborum is seen medial to the aponeurosis of the tranversus abdominis
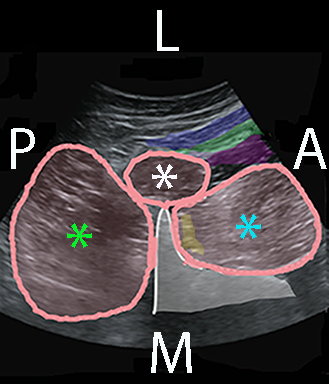
With a slight caudad tilt of the probe the body and transverse process (TP) of vertebral body L4 can be seen surrounded by the quadratus lumborum (QL) at the tip of the TP, erector spinae posterior to the TP and psoas major anterior to the TP
This is the “shamrock sign” – the treefoil of the stem of the TP surrounded by the three muscle “leaves”
TP of L4 (gray) surrounded by the QL (white asterix), psoas major (cyan asterix), and erector spinae (green asterix). The lumbar plexus (yellow shadow) is just anterior to the TP. The external and internal obliques and the transversus abdominis are blue, green and purple. A = anterior, P = posterior, M = medial and L = lateral
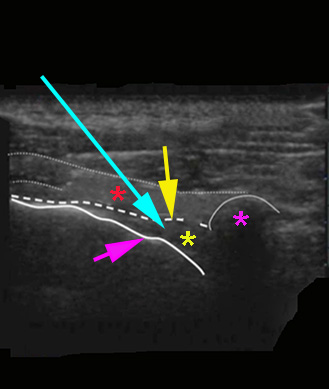
The pleura is visible as a hyperechoic line with “pleura sliding” in synchrony with respiration
This is different from the rib that has an anechoic acoustic shadow and no lung sliding
The needle is advanced with real-time in-plane technique and aims at the triangular thoracic paravertebral space underneath the internal intercostal membrane and the needle tip should be placed right next to the anechoic acoustic shadow of the transverse process; a “pop” is often felt when the needle tip penetrates the internal intercostal membrane
After assuring negative aspiration for blood 15-20 mL of local anaesthetic is injected. The TPS is seen to expand and push the pleura downwards
The local anaesthetic should be injected into the anterior part of the TPS anterior to the endothoracic fascia; this assures that the local anaesthetic spreads longitudinally inside the TPS and that sympathectomy is produced