B-lines may be found throughout the lungs bilaterally
Spared areas with no B-lines are often seen (as opposed to cardiogenic pulmonary oedema)
The visceral pleura may also be affected and can appear thickened and fragmented
B-lines may be found throughout the lungs bilaterally
Spared areas with no B-lines are often seen (as opposed to cardiogenic pulmonary oedema)
The visceral pleura may also be affected and can appear thickened and fragmented
Patients with exacerbation in chronic obstructive pulmonary disease (COPD) or asthma do not have interstitial syndrome
Hence, in acute admitted patients with dyspnoea, LUS can be used as a tool to differentiate between cardiogenic and pulmonary causes of dyspnoea
The finding of interstitial syndrome is a powerful diagnostic tool in diagnosis of pulmonary edema
FLUS is very sensitive for detecting interstitial oedema. Consequently, a FLUS examination with no signs of interstitial syndrome can be used to rule out conditions such as cardiogenic pulmonary oedema
Any condition with universally increased density in the lungs may cause universally multiple B-lines and therefore the interstitial syndrome
In adults the following conditions have been described as causes of interstitial syndrome:
– Cardiogenic pulmonary edema
– Non-cardiogenic pulmonary edema (e.g. fluid overload, renal failure)
– Interstitial lung diseases
– Viral pneumonia
– Bacterial pneumonia
– ARDS
– Acute chest syndrome
– Drowning / near-drowning
– Lung contusion
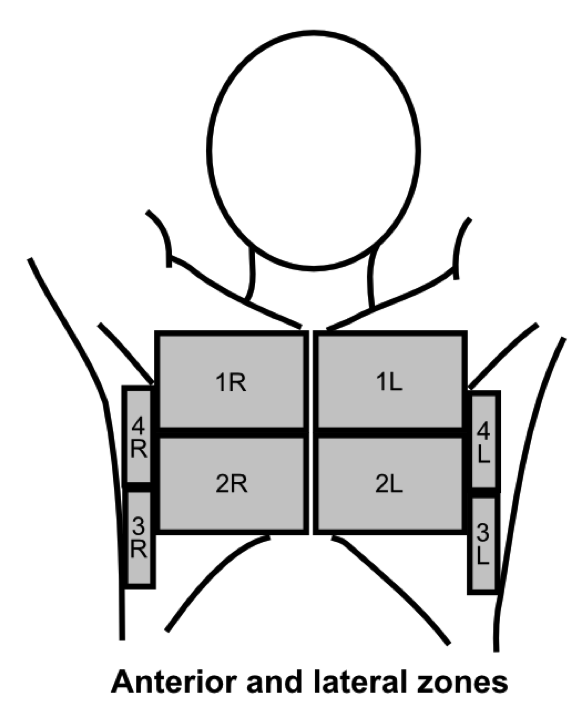
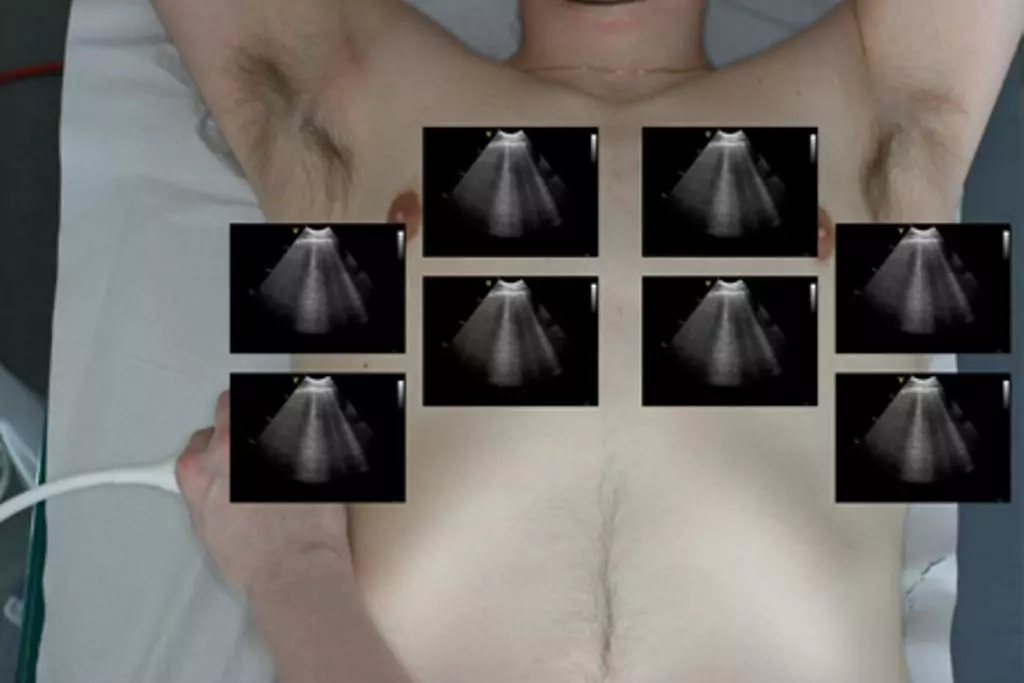
Using the scanning technique described in the examination technique module, with two anterior, two lateral and three posterior scanning zones, the criteria for IS is the presence of both of the following:*
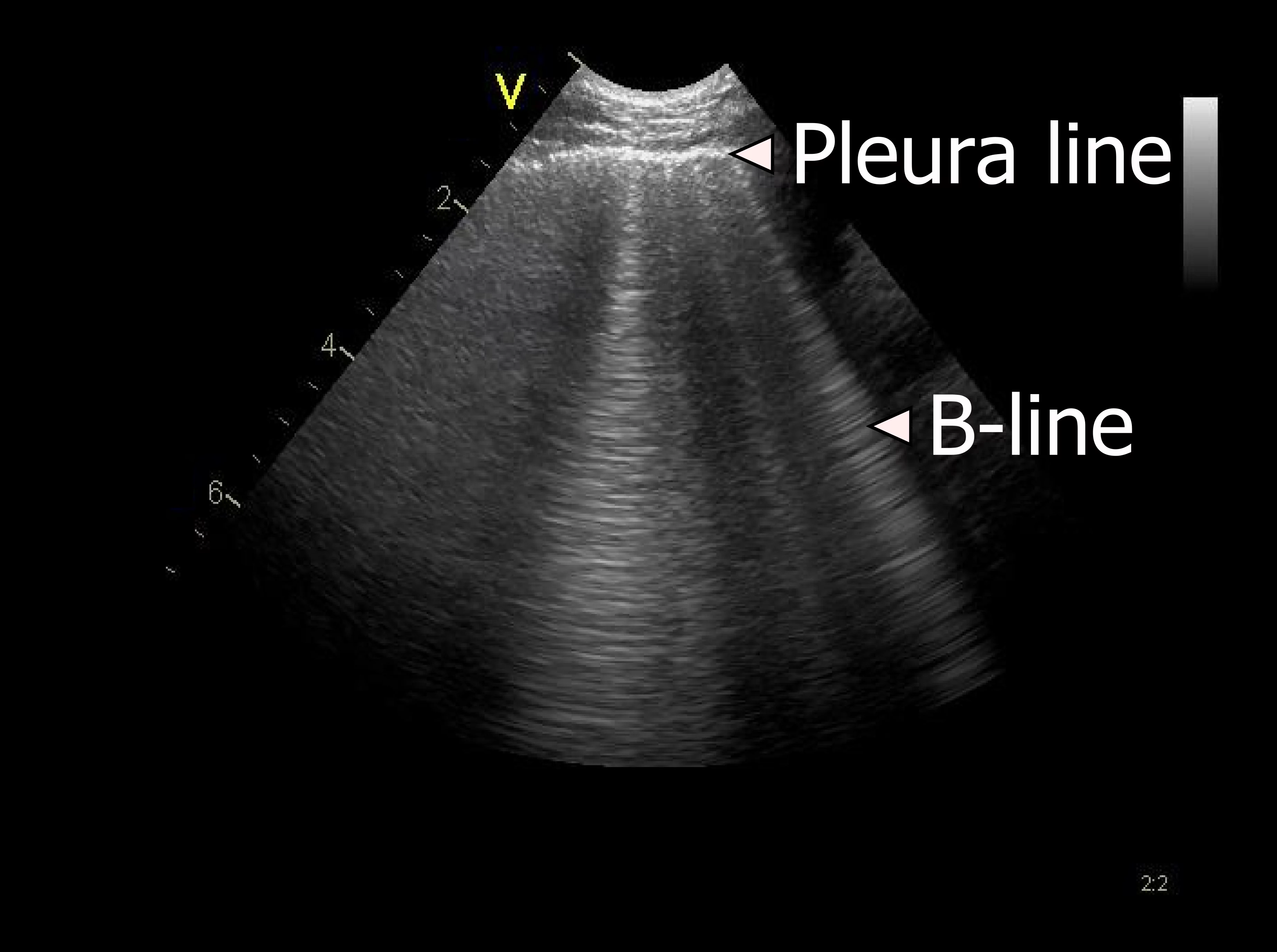
1: A positive scanning zone is defined by the presence of three or more B-lines in a longitudinal plane between two ribs
2: When scanning the anterior and lateral zones, two or more of the zones have to be positive on each side
* Volpicelli, G., et al., “International evidence-based recommendations for point-of-care lung ultrasound”, Intensive Care Med, 2012, 38(4): p. 577-91
Multiple B-lines can in some diseases be seen almost universally when scanning both lungs. This finding is often referred to as the interstitial syndrome (IS
The occurrence of multiple, isolated B-lines can both be normal and a pathological sign
In studies approx. 25% of patients with normal chest imaging have multiple B-lines in the lower lateral intercostal space
The presence of focal areas with multiple B-lines can also be seen in any disease with a localised increased density of the lung tissue such as pneumonitis, atelectasis, pulmonary contusion, pulmonary embolism, pleural disease and malignancy

Other vertical hyperechoic artefacts may mimic the B-line, but these artefacts always become less hyperechoic or completely fades out
In comparison, B-lines never fade out and can be visualised the entire way to the bottom of the field of view
Since these artefacts quickly fade out and cannot be visualised the entire way to the bottom of the field of view, they do not represent B-lines
For this purpose the presence and zonal distribution of B-lines is used
B-lines are an indirect marker of lung disease
B-line artefacts occur when the density of the lung has increased as for example in interstitial oedema or pulmonary fibrosis
Lung ultrasound can be used for diagnosing common pathology in the thorax
Pneumothorax can be ruled out with simple and easily obtained imaging. Ruling in pneumothorax is often more difficult
Pleural effusion are easily identified with the correct technique
Lung ultrasound helps discern interstitial syndrome from other causes of respiratory failure
